Episode 9: Nutritional Deficiencies and Dietary Supplements – Part 2
Podcast: Play in new window | Download
Episode 9: Nutritional Deficiencies and Dietary Supplements – Part 2
- Answering the questions about use of nutritional supplements:
- How do we recognize/suspect the need?
- When should we use nutritional supplements?
- In order to better recognize and understand nutritional deficiency, it helps to review some basics of nutritional research
- Methods: Experimental and observational study used to identify deficiency syndromes
- Often begun with the observation that certain foods influenced active disease processes
- Limes used to prevent and treat scurvy
- Efforts directed toward identifying the beneficial substance(s) in those foods.
- The primary focus of the early research was on vitamins
- Philosophy of Nutritional Scientists: Synthetic Reproduction of ‘Active’ Ingredients
- Early research failed to recognize the chemical complexity of foods
- Assumed that foods are simple mixtures of a few easily identified chemical constituents, which, through modern chemistry, can be easily reproduced
- Nutritional Research: Defining Nutrient Deficiencies
- (introduced this idea in episode 2 when describing how “essential” nutrients are identified for pet food.)
- Defining disease syndromes of nutrient deficiency relies on the total exclusion of a single nutrient, such as a vitamin, over short-term.
- The manipulated diet produces the classical signs of disease associated with the absence of that nutrient.
- Understanding nutritional studies
- Observational (dietary intake)
- Diets containing large amounts of foods high in β-carotene (yielding high blood levels of β-carotene) have been associated with decreased risk of cardiovascular disease and several types of cancer
- Intervention trials (supplementation)
- Different vitamin sources affect outcomes of clinical studies
- Supplementation trials may yield contradictory results
- Example: Synthetic β-carotene supplementation
- Observational (dietary intake)
- Nutritional Research-The Key to Understanding ‘Conflicting’ Results
- The Case Against Vitamins Wall Street Journal March 20, 2006 p. R1, R3
- http://www.mythyroid.com/documents/WSJVitamins.pdf
- http://online.wsj.com/article/SB114235146814497776.html
- Prevalence – 70% of households buy vitamins
- $7 Billion spent on vitamins in 2005
- Rationale
- Boost immune system
- Protect heart
- Decrease risk of cancer
- Results
- “May be doing more harm than good”
- Detrimental effects
- Cancer promotion
- Increased risk of heart failure
Last year, Johns Hopkins University researchers in Baltimore published a shocking finding. After reviewing the data from 19 vitamin E clinical trials of more than 135,000 people, the analysis showed high doses of vitamin E (greater than 400 IUs) increased a person’s risk for dying during the study period by 4%. Taking the vitamin E with other vitamins and minerals resulted in a 6% higher risk of dying.
Since the analysis was published, another study of about 9,500 patients evaluated long-term use of 400 IUs of vitamin E daily. The study didn’t show any statistically meaningful differences between vitamin users in terms of cancer, heart attacks or stroke, but the vitamin E takers had a 13% higher risk for heart failure.
“The psyche of the U.S. population is that a nutraceutical can’t be harmful and might be helpful, so why not take it?” says Dr. Klein. “That thinking is just not correct.
- What is going on?
- “Nobody knows why high doses of vitamins taken as pills might cause harm”
- “What is clear, however, is the important role a healthful diet plays in preventing illness”
- The critical difference is that vitamin complexes and phytochemicals found in food are fundamentally different than isolated pharmaceutical doses of vitamins.
- Observation vs. Intervention: Detrimental Effects of Synthetic Beta Carotene
- β-carotene initially appeared to be the associated link between lowered cancer risk and dietary intake of fruits and vegetables (observation)
- No benefits have been found with β-carotene supplementation in randomized trials (intervention)
- CARET (β-carotene and Retinol Efficacy Trial)
- Vitamin A (retinol) and synthetic β-carotene supplements
- 18,314 men and women
- Study stopped 21 months early
- No protective benefit
- Increased risk of lung cancer and higher mortality in the intervention group
- ATBC (α-tocopherol, β-carotene cancer prevention study)
- Synthetic dl-α-tocopherol and synthetic β-carotene supplements
- 29,133 male smokers in Finland
- Increased cancer risk with supplementation
Although studies have suggested an association between diets rich in beta carotene and vitamin A and a lower risk for many types of cancer, the supplements taken in pill form have proved risky.
The 1994 Finland study of smokers taking 20 milligrams a day of beta carotene showed an 18% higher incidence of lung cancer among beta carotene users. In 1996, a study called Caret looked at beta carotene and vitamin A use among smokers and workers exposed to asbestos. The trial was stopped when the participants taking the combined therapy showed a 28% higher risk for lung cancer and a 26% higher risk of dying from heart disease.
More recently, a 2002 Harvard study of more than 72,000 nurses showed that those who consumed high levels of vitamin A from foods, multivitamins and supplements had a 48% higher risk for hip fracture than nurses who had the lowest intake of vitamin A. Notably, nurses who ate a lot of foods high in vitamin A also had higher risk, possibly indicating that too many foods are:
- now fortified with the vitamin. Milk, margarine and breakfast cereals are fortified with vitamin A. High intake of vitamin A has also been associated with a higher risk of birth defects.
(The Case Against Vitamins Wall Street Journal March 20, 2006 p. R1, R3)
- Dietary vs. Supplemental Phytochemicals/Antioxidants
- Why are lower doses of dietary antioxidants beneficial, but higher doses of supplementary antioxidants not offer expected levels of protection against free radicals?
- Synthetic Reproduction of ‘Active’ Ingredients
- Synthetic chemical substances often do not convey the identical health benefits as the same compound when consumed with the parent food
- More complex than can be synthesized and reproduced in the laboratory
- Complexity of food biochemistry and physiological impacts continue to be poorly understood
- Balanced intake of synergistic components
- Balanced absorption (lack of interference from isolated synthetics)
- Natural nutrient forms (compatible with animal enzyme systems)
- Lack of induction of detoxification enzyme systems that enhance elimination of supplemental nutrients
- Gene regulating effects on intracellular detoxification enzyme systems affecting phase I and phase II balance
- In healthy organisms, there is a balance between oxidants and various antioxidants
- Reactive oxygen species are not solely harmful but are involved in many defense reactions of the cells
- “High levels of antioxidants may disturb these reactions with unpredictable and unexpected consequences…”
{Rautalahti M, Virtamo J, Haukka J, et al. The effect of alpha-tocopherol and beta-carotene supplementation on COPD symptoms. Am J Respir Crit Care Med 1997 Nov;156(5):1447-1452.}
- “Food is an extremely complex matrix consisting of thousands of natural components, many of which have not been characterized.”
{Rasooly L, Rose NR. Food toxicology and immunity. Nutrition and Immunology: Principles and Practice Gershwin, German, Keen Eds. 2000}
- Complexity of Food Biochemistry: Biologically Active Compounds
- “Food is more than a source of calories and nutrients to prevent deficiency diseases. It represents a matrix of interacting substances that influence biological response modifiers, the functional aspects of physiology. By manipulating the diet appropriately and using nutritional pharmacology where necessary, dysfunctional patterns of intercellular communication can be modified to establish the physiologic patterns of health.”
{Bland, J. 2000 Seminar Series Syllabus: Nutritional management of the underlying causes of chronic disease. P. 161-2
- Complexity of Food Biochemistry: “Herbal Remedies” and “Medicinal Botanicals”
- Currently recognized that there are a host of “nonnutritive” components of plants that can have active roles in disease prevention
- “Biological response modifiers”
- Some animal products, not traditionally thought of as foods, also can have active roles in disease prevention
- Bear gallbladder, ginko lizard, deer antler, shark fins
{Gundling K, Borchers A, Gersshwin ME. Nutrition, immunity, and alternative medicine.}
{Nutrition and Immunology: Principles and Practice 2000 Gershwin, German, Keen}
- There is a fundamental difference between the biological action of a pure chemical and the same chemical in a plant matrix
- Synergy
- The biological action of the chemical mixture is greater than the sum of the actions of the mixture’s components (“The whole is greater than the sum of the individual parts”)
- Certain plant compounds with minimal or no biological activity can improve stability, solubility, or bioavailability of active components
- Synergy
{Principles and Practice of Phytotherapy: Modern Herbal Medicine. Mills S, Bone K. 2000}
- More than ‘antioxidants’
- Interaction with specific receptors
- Modulate expression of genes regulating specific enzyme systems
- A common effect of numerous identified phytochemicals is regulation of gene expression for detoxification enzyme activity
- Up-regulation of phase II
- Down-regulation of phase I
- Alteration of antioxidant status within cells
- Enhance immune responses
- Modulate circulating hormone concentrations
- Modify inflammation via receptor-mediated effects on expression of specific genes
- Cyclooxygenase-2
- PGE-2
- Switching off/on specific genes involved in cell growth, proliferation, and death
- Inhibition of cell proliferation/induction of apoptosis
- Tumor suppressor genes
- Oncogenes
- Partial deficiency over long term is very different than complete deficiency over short period
- Typically is not single vitamin or nutrient, but combination of several nutrients operating in conjunction
- What clinical signs might be expected with long-term partial deficiencies?
- Example: The vague signs of decreased immune function can be a result of partial deficiency of:
- Selenium, zinc, vitamin A, copper, omega 3 fatty acids, taurine, and glutamine
- Other chronic diseases such as cancer, arthritis, allergies, cardiovascular disease, reproductive problems, and neurodegenerative disorders/ cognitive dysfunction may have nutritional origins
- Example: The vague signs of decreased immune function can be a result of partial deficiency of:
- Acknowledgement of Partial Nutrient Deficiency in Disease JAMA June 2002
- “Classic” deficiency syndromes not seen in Western societies
- Scurvy, beriberi, rickets
- ‘Sub-Clinical’ deficiencies common
- “Sub-Optimal” vitamin status associated with many chronic diseases
- Cardiovascular disease, cancer, osteoporosis
- Physicians must learn to recognize those with poor nutrition or reasons for increased vitamin needs
- Blood, serum, and red blood cell measurements are not reliable indicators of this type of deficiency
- They recommend a daily multivitamin
- Unfortunately, “the science of vitamin supplementation for chronic disease is not well developed”
- Dietary recommendations (RDA)
- Population-based data
- Minimums
- Designed to avoid well-characterized deficiency syndromes
- When available scientific information is incomplete, RDA estimates can be wrong
- As knowledge changes, recommended intakes change
- Folate
- Metabolic, environmental, and genetic factors along with pathologic conditions may alter individual nutrient requirements
- As knowledge changes, recommended intakes change
- “Classic” deficiency syndromes not seen in Western societies
- “Sub-Clinical” Deficiency Syndromes: Vitamin A
- History
- 1800’s effects of a deficient diet
- 1900’s identified the foods that treated the deficiency syndrome (What foods, not Why this food?)
- Identified substances in the foods: carotenoids and vitamin A
- 1947 successful, cost-effective synthesis of ‘vitamin A’
- But…vitamin A refers to a group of fat-soluble substances called retinoids
- Vitamin A Status: The “sub-clinical” deficiency
- No ocular lesions
- Not ‘classic’ signs
- Increased mortality
- Decreased cellular integrity
- Decreased immune function
- Difficult to diagnose
- “Between the extremes [toxicity, total depletion] is a relatively large zone where status cannot be easily quantified by currently available techniques.”
- History
{Prevention of Micronutrient Deficiencies: Tools for Policymakers and Public Health Workers (1998). http://www.nap.edu/openbook/030906029X/html/106.html, The National Academy of Science}
- “Sub-Clinical” Deficiency Syndromes: Folate/B12
- Dementia & Alzheimer’s-like syndrome in people
- B12 important for nerve myelination and fat/protein metabolism
- Atrophic gastritis = ↓ gastric acid
- ↓protein digestion and ↑bacterial growth
- ↓free B12 from protein and ↑metabolism of existing free B12
- “Sub-clinical” B12 deficiency
- Clinical syndrome of confusion and disorientation
- No evidence of megaloblastic anemia (classical B12 deficiency)
- Dementia & Alzheimer’s-like syndrome in people
{Cyberounds: The Subtle Presentation of Vitamin B12 Deficiency Russell, RM, Mason JB 8/96 http://www.cyberounds.com/conferences/nutrtion/conferences/0896/conference.html
“…it is now apparent that degrees of folate depletion that are not severe enough to cause megaloblastic anemia can have deleterious effects on the health of affected people. For example, mild decrease in folate status can lead to elevated levels of homocysteine in the blood which is thought to be an independent risk factor for arteriosclerotic vascular disease.”
{Cyberounds: Nutritional Issues In and a Promising New Treatment of Inflammatory Bowel Disease Russell, RM, Mason JB 10/96}
- Neurodegenerative Disorders & Cognitive Dysfunction
- Canine C.D. estimated to affect 47% of dogs age 11-12 years, 86% of 15-16 year old dogs
- Alzheimer’s disease and CD in dogs share many similarities
- Same regions of the brain affected
- Beta-amyloid plaque formation
- Similar neurotransmitter dysfunction/imbalance
{Ruehl WW, Hart BL et. al. L-Deprenyl therapy for canine cognitive dysfunction Kirk’s Current Veterinary Therapy XIII 2000 pp.53-57
- “The risk of PD [Parkinson’s disease], however, was significantly reduced among men and women with high intake of dietary vitamin E (from foods only). The reduction in risk of PD associated with high dietary vitamin E intake suggests that other constituents of food rich in vitamin E may be protective.”
{Zhang SM, Hernan MA, et. al. Intakes of vitamins E and C, carotenoids, vitamin supplements, and PD risk. Neurology 2002 Oct 22;59(8):1161-9.}
- “Diets rich in fruits and vegetables have been shown to improve human well-being and to significantly delay the development of pathologic processes, including neurodegenerative disorders.”
{Martin A, Cherubini A, Andres-Lacueva C, Paniagua M, Joseph J Effects of fruits and vegetables on levels of vitamins E and C in the brain and their association with cognitive performance. J Nutr Health Aging 2002;6(6):392-404.}
- “Nutrition may be useful for preventing dementia…”
{Otsuka M, Yamaguchi K, Ueki A Similarities and differences between Alzheimer’s Disease and vascular dementia from the viewpoint of nutrition. Ann N Y Acad Sci 2002 Nov;977:155-61.}
- “Sub-Clinical” Deficiency Syndromes: Glutamine
- Considered to be ‘conditionally’ essential
- Demand may exceed synthetic capacity any inflammation or disease condition
- Essential for the entire body
- Immune function – enteric and systemic
- Tissue repair
- Enterocytes
- Essential for preservation and normalization of:
- small bowel villus morphology
- intestinal permeability
- enterocyte function
- intestinal healing
- Prevention of bacterial translocation
- Essential for preservation and normalization of:
{Small Animal Clinical Nutrition 4th Ed p. 81}
{Allen TA, Hand MS. Conditionally essential nutrients: antioxidant nutrients and glutamine. Kirk’s Current Veterinary Therapy XI Small Animal Practice 1992 pp. 40-43}
- High heat processing of commercial pet foods destroy large amount of glutamine leaving them depleted
- Known to be deficient in cancer patients fed commercial dry/canned diets
- Supplementation shown to be beneficial for quality of life and healing with chemotherapy and radiation therapy
- Commercial diets…How much is really in there?
- Deficiencies despite an “adequate” amount in a “balanced” diet?
- Role in IBD?
{Small Animal Clinical Nutrition 4th Ed p. 81}
{Ogilvie, G. Complimentary/integrative cancer care: fact or fiction? North American Veterinary Conference lecture notes Jan. 22, 2003}
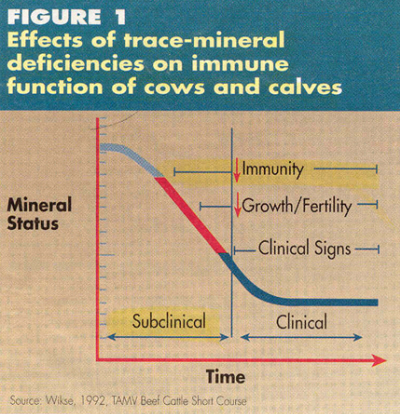
- Examples of Immune Dysfunction From “Subclinical” Deficiencies: Zinc
{Verdon DR Study: Zinc common element deficient in forages. DVM Newsmagazine, June 1996, p. 1F}
- The graph highlights the area of “subclinical” disease
- In this range, the serum zinc is within the reference ranges and the deficiency is undetectable by conventional measures
- Compromised immune function and impaired fertility become apparent
- The appearance of classical signs of dietary zinc deficiency (such as zinc dermatosis) do not appear until later in the course of developing deficiency
- Bioavailability – interfering substances affect nutrient absorption and utilization
- This highlights several important concepts which have been mentioned and deserve repeating:
- Real-world nutritional deficiencies rarely appear as classical nutrient deficiency syndromes
- Real-world nutritional deficiencies frequently consist of subtle signs of diminished immune competence and susceptibility to infections, cancer, immune mediated disease, etc.
- Real-world nutritional deficiencies are usually not easily detected by a blood test
- Malnutrition and Susceptibility to Disease
- Commonly thought that malnutrition diminishes host immune responses and is responsible for increased susceptibility to disease
- Famines followed by epidemics of infectious disease
- Nutritional status of the host can affect the genetic expression of a pathogen, changing a normally avirulent organism into a virulent one
- Examples:
- Measles generally mild with few complications in unvaccinated individuals when normal vitamin A status
- Deficiency of vitamin A associated with severe disease and high mortality
- Increased severity of respiratory syncytial virus infections when vitamin A deficient
- Malnourished mosquitoes may be more susceptible to certain viruses and may transmit more virus when feeding
- Experimentally shown with LaCrosse Virus
- Enhanced pathogenesis associated with increased oxidative stress
- Oxidative damage to viral genome
- Diminished clearance of virus by host immune system
- Increased incidence of mutations in virus
- Measles generally mild with few complications in unvaccinated individuals when normal vitamin A status
- Commonly thought that malnutrition diminishes host immune responses and is responsible for increased susceptibility to disease
- The bottom line –
- Food is much more complex than synthetic vitamins
- Many supplements do not feed the body effectively ( and many are dangerous)
- Nutritional deficiencies occur (!)…. and our index of suspicion should be higher
- In other words, going back to episode 1, we should be asking whether every illness has a nutritional component
- Episode 10 will discuss more about what type of supplementation should be used to feed the body according to its natural design
Leave a Reply